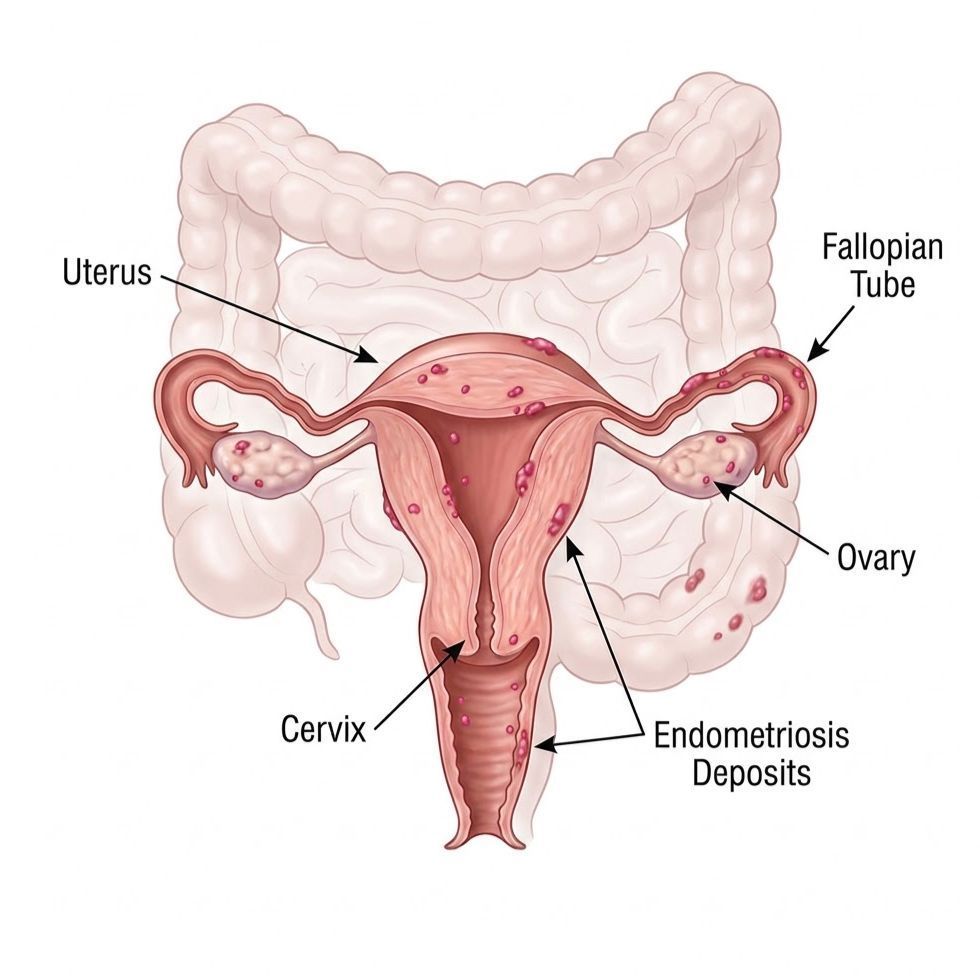
What endometriosis actually is
Endometriosis is a condition in which tissue similar to the lining of the uterus grows outside the uterus. As the WHO describes it, this tissue causes inflammation and scar tissue, most often in the pelvis, and sometimes elsewhere in the body. It affects an estimated 10% of reproductive-age women worldwide, about 190 million people. It is a chronic disease, and there is currently no cure, though symptoms can be managed well with the right care.
Common symptoms
Pain severe enough to interfere with school, work, or daily life is not something to push through quietly. Common symptoms include:
- Painful periods (dysmenorrhea)
- Pain during intercourse (dyspareunia)
- Pain during bowel movements or urination
- Heavy menstrual bleeding
- Chronic pelvic pain that continues after your period ends
- Bloating, nausea, or fatigue
- Difficulty getting pregnant alongside any of the above
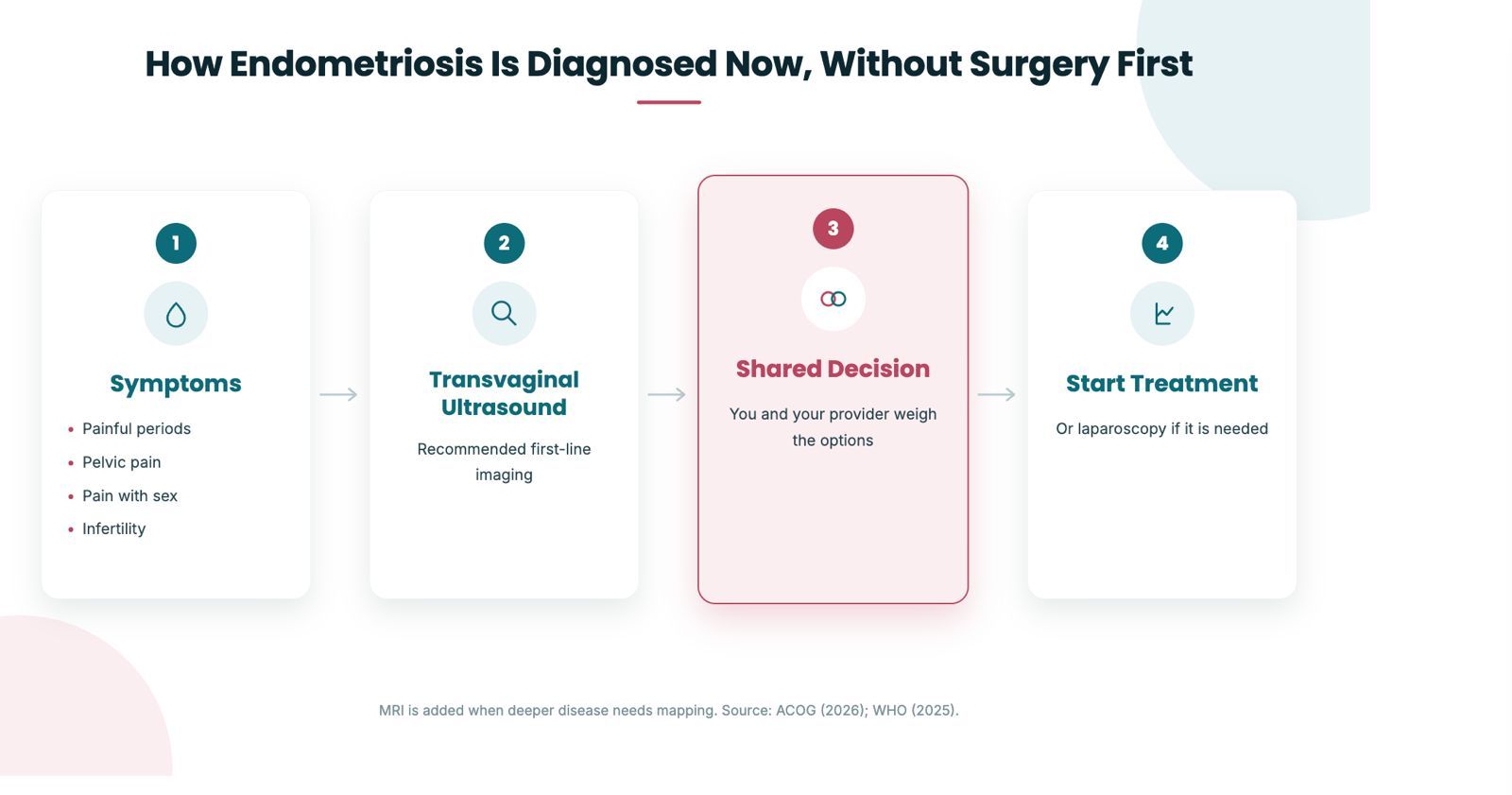
Why diagnosis took so long, and why that is changing
The old model treated laparoscopy as the only way to be sure. Because surgery carries risk, cost, and access barriers, many women waited years while their pain was normalized. The WHO puts the average time for diagnosis at 4 to 12 years. ACOG's clinical practice guideline shifts the entry point: clinicians should suspect endometriosis from symptoms, and can start treatment after a clinical diagnosis, rather than requiring surgery first. The WHO now agrees that a clinical diagnosis may be made from symptoms and imaging, and that surgery is not necessarily required before starting treatment.
What does NOT diagnose endometriosis
There is currently no blood test to diagnose endometriosis. ACOG strongly recommends against using blood, urine, or other biomarker tests to diagnose the condition, because none of them are as accurate as symptom-based assessment, imaging, or surgical confirmation. If you see a direct-to-consumer test marketed as a way to confirm endometriosis from a blood or saliva sample, current guidance does not support it as a diagnostic tool.
01
When is surgery actually needed?
Surgery is no longer required simply to diagnose endometriosis. Under the latest ACOG guidance, it is reserved for specific situations:
- Severe, uncontrolled symptoms that do not respond to medication
- Deep infiltrating endometriosis lesions
- Ovarian endometriosis (endometriomas, sometimes called chocolate cysts)
- Fertility-related indications, such as blocked fallopian tubes before IVF
02
How endometriosis is treated
Treatment is individualized. It depends on symptom severity, your preferences, side effects, and whether you are trying to become pregnant. Based on WHO and ACOG guidance, the main options are:
- Pain relief: non-steroidal anti-inflammatory drugs such as ibuprofen or naproxen
- Hormonal therapy: combined hormonal contraceptives, progestins (including the hormonal IUD), or GnRH analogues
- Surgery: minimally invasive removal of lesions, adhesions, and scar tissue when medication is not enough
- Fertility care: ovulation induction, intrauterine insemination, or IVF for those trying to conceive
- Whole-person support: physiotherapy and cognitive behavioral therapy can help reduce pain and improve quality of life
03
Where surgery still fits
The new guidance does not mean surgery disappears. It means surgery is no longer the price of admission for being believed. When surgery is the right step, it can often be done through minimally invasive techniques, including daVinci robotic gynecologic surgery, which is designed for precision and shorter recovery. The point is sequencing: you should not have to wait for an operation to start feeling better.
04
The honest limits.
A clinical diagnosis from symptoms and imaging is not as accurate as visual confirmation at laparoscopy, so some uncertainty can remain. Ultrasound can miss superficial disease, which is why a normal scan does not fully rule endometriosis out. There is no cure, and symptoms can recur even after successful treatment. None of this is a reason to wait years for care. It is a reason to start the conversation now.
Getting evaluated in Plymouth Meeting
Evaluation can begin with your history and an in-office pelvic ultrasound, using wireless ultrasound technology at the point of care. Dr. Hema Jonnalagadda, a Fellow of the American College of Obstetricians and Gynecologists, builds a plan around your symptoms and your goals, whether that is pain relief, fertility, or both. You do not have to prove your pain through surgery to be taken seriously.
Frequently asked questions
About the author & sources
Dr. Hema Jonnalagadda, MD, FACOG, is the founding physician of Advocare Montgomery Gynecology in Plymouth Meeting, PA, and a Member of The Menopause Society. She provides evidence-based women's health care from adolescence through menopause.
This article is for general education and is not a substitute for individual medical advice. If you are in severe pain or have new or concerning symptoms, please consult your provider.
Sources (primary)
- World Health Organization. Endometriosis fact sheet (updated October 15, 2025). https://www.who.int/news-room/fact-sheets/detail/endometriosis
- American College of Obstetricians and Gynecologists. Clinical Practice Guideline on evaluation and diagnosis of endometriosis, Obstetrics & Gynecology (2026). https://www.acog.org
- World Health Organization. Infertility fact sheet (2025). https://www.who.int/news-room/fact-sheets/detail/infertility